Unless you live in a cave without any access to the internet, television or print media, you have likely been bombarded with ads promising a new body, stellar fat loss, amazing muscle definition and a super slim, sculpted body in no time. The most enticing aspect of these ads is the promise that a new, slimmer you can be accomplished without altering your eating or exercise habits; just take a pill.
If it were that simple, everyone would be in shape, weight loss would be simple and obesity would not be the growing public health problem that it is. With so many products out there and all of the amazing claims and testimonials, surely something must work, right? While it is true that the majority of wild claims and promises are ridiculous and in many cases simply false, there are ways that supplementation can make fat/weight loss easier or quicker.
The goal of incorporating a dietary supplement or drug into a weight loss program is to assist the participant in complying with the daily routine that leads to weight reduction. The dieter would cease supplementation once the weight goal is reached, or when they have their daily routines under control to continue making progress without the supplements.
If a fat loss product is added to one's daily routine and a change in body composition occurs over time that is greater than it would be without the product, then one can reasonably say that something about the product seemed to work. When fat loss products do work, it is by its affects on one or more of the following:
- Appetite- decreased desire to eat or increased/longer feeling of fullness (leading to fewer calories eaten)
- Increased energy expenditure- more calories are burned through thermogenesis (use of extra calories as heat rather than fat storage) or increased daily movement (stimulants tend to make people move more because they have more "nervous energy")
- Decreased calorie absorption- portions of dietary fat or carbohydrate are rendered "unabsorbable" and these calories, though eaten, are not added to the body
Any fat loss supplement must work in one or more of the previous three ways regardless of its marketing and word of mouth. If not, then it truly is magic, and when it comes to the body and weight loss, magic doesn't cut it. Let's look at how dietary supplement components can affect appetite, energy expenditure and caloric absorption.
Appetite
Appetite is defined as the desire to eat. The regulation of appetite is influenced by a great many things, including the interplay between the digestive tract, your body fat stores and the brain.(1,2,3) The internal environment of the body is very dynamic, with changes occurring in the levels of amino acids, carbohydrate and glucose, fatty acids, enzymes and hormones throughout the day. A change in any one of these factors (and thousands more) can affect one's appetite. In addition to internal factors, appetite is shaped and influenced by your upbringing and environment. Family gatherings, holidays, time of day, smells . . . all of these can have strong associations with food (especially "comfort foods") and can affect eating behavior.(4,5,6,7,8) Not convinced? What happens when you smell freshly baked chocolate chip cookies? Do memories come rushing into your head? It is fair to say that today very few people make the decision to eat based strictly upon hunger (which is defined as a NEED for nourishment). Fried appetizers and dessert are not biologically necessary for survival, but a learned, reinforced behavior.
Appetite, Satiety and Pharmaceutical Intervention
The main feeding center in the brain is the hypothalamus.(1)i It receives and sends signals that determine if our appetite is stimulated or suppressed (often referred to as satiety). While there are myriad factors that influence these feelings, two hormones and their effect on neurotransmitters, appetite and weight control have emerged as key players. They are Leptin and Ghrelin. Leptin, discovered in 1994, is a hormone released from fat tissue that helps signal satiety.(9) The drug Sibutramine is used to mimic the actions of Leptin, maintaining higher levels of Serotonin, a neurotransmitter that signals satiety and feelings of well being.(10) Ghrelin, a hormone secreted from the stomach, is essentially the evil twin of Leptin. As Ghrelin levels rise, the hypothalamus is stimulated to increase appetite.(11) Ghrelin levels will rise prior to meals and lower afterwards, following this cyclical pattern throughout the day. In those who are obese, the peaks tend to be higher and stick around longer. Drug therapy to reduce appetite has tried to inhibit Ghrelin secretion.
Additional appetite regulators include gut peptides that are released in response to food intake, such as cholecystikinin (CCK), which is stimulated by protein and fat intake as well as pancreatic polypeptide (PP), peptide tyrosine-tyrosine (PYY) and glucagon like peptide-1 (GLP-1).(12,13) Even the presence of food in the stomach appears to signal fullness. The interplay of all of the factors affecting appetite is exceptionally complex and can vary person-to-person, making a simple approach to obesity and weight loss difficult. Additionally, there are so many checks, balances and feedback systems in the body that several other systems can take over to pick up the slack if one hormone or neurotransmitter is changed.
The Natural Approach
There is no question that drug intervention can be helpful, but the side effects are often as risky as the condition they hope to treat. This has led to the search for natural compounds that can mimic the actions of drugs, but without the side effects. Following are some of the current natural solutions that hold promise for those trying to lose weight.
Fiber is one of the cheapest, easiest and healthiest ways to eat fewer calories, feel full sooner and stay full longer.(14) Dietary fiber adds bulk to meals and provides a non-digestible aspect to the diet (meaning no calories!). Fiber also slows the release of carbohydrate and the emptying of food from the stomach. There are products that utilize fiber extracts to help accomplish this. One of these is citrus pectin, a soluble fiber (glucose-polysaccharide) obtained from citrus peels that slows the emptying of food from the stomach, increasing satiety. Additionally, it may have cholesterol lowering benefits.(16)
Caffeine and caffeine-containing herbs (such as yerba mate, guarana seeds, green tea leaf extract and cayenne fruit). Caffeine belongs to a group of compounds called methylxanthines and these compounds have a small effect on reducing appetite. Where caffeine really shines is in its ability to magnify and prolong the effects of other substances that may have a greater impact on appetite.(17,18,19,20,21,22,23)
Caralluma fimbriata (CF) is an extract from an edible succulent cactus that has a long and safe history of use as an appetite suppressant, similar to the supplement Hoodia gordonii. Unlike Hoodia, CF has been researched for safety and efficacy producing positive results.(24) CF may suppress appetite by amplifying the signaling of energy sensing functions in the hypothalamus. Additionally, CF may act much like another common appetite suppressant, hydroxycitrate (HCA), by blocking citrate lyase (an enzyme responsible for converting excess carbohydrate into fat). This prevents fat accumulation and redirects extra energy/calories to glycogen stores (the storage form of carbohydrate in the liver and muscle), which may also improve satiety.(25,26)
Increased Energy Expenditure
There are two ways that added substances can increase a person's 24 hour energy expenditure (24hr EE). Either the substance makes the user feel more "energetic" or "antsy", motivating them to move (this is called spontaneous physical activity - SPA) or it causes internal adaptations that increase the use of energy for heat rather than storage as fat, or it activates futile, wasteful energy cycles (called thermogenesis). Either way, when the day is over, you burned more calories.
There are several natural compounds that increase energy expenditure and fat loss. The oldest, safest and best known is Caffeine/Methylxanthines (see caffeine-containing herbs above) and Green Tea Extract (EGCG).
Caffeine has been shown repeatedly to increase energy expenditure, alertness and fat oxidation (the use of fat as fuel), improve mood and positively impact almost any type of performance parameter tested.(17,18,19,20,27,28,29) As stated earlier in this article, it is also used to enhance and prolong the effects of other ingredients that can aid in weight loss.
EGCG has gained popularity as a wonder ingredient as of late, showing benefits in increasing fat utilization and energy expenditure, improving many of the health parameters of metabolic syndrome (blood pressure, LDL/HDL cholesterol, insulin sensitivity and glucose tolerance) and reducing the risk of cancer.(30,31,32,33) It is the polyphenols and catechins that are associated with the beneficial effects. And as an added bonus, those who used EGCG for weight loss also noted improved mood.(33)
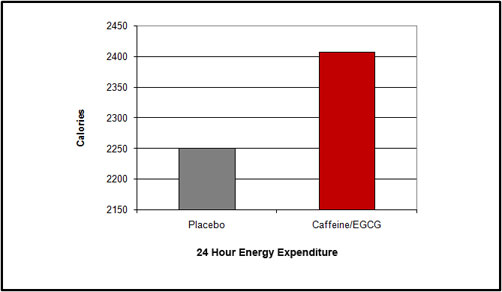
FIGURE 2: Studies demonstrate at least a 10% increase in 24 hour EE or equivalent to 157 more calories burned in the caffeine/EGCG group (Average test subject’s weight 173 lbs).
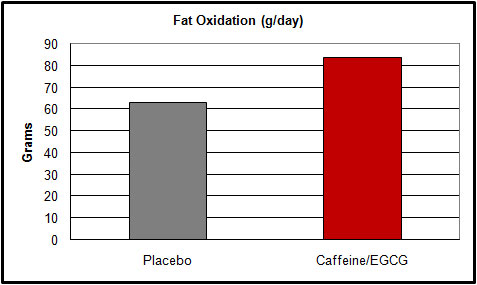
FIGURE 3: Approximately 20 grams more fat daily was oxidized by the supplemented group.
Capsaicin from Cayenne fruit can stimulate sympathetic nervous system activity (energy and the fight or flight response), promote the secretion of catecholamines (epinephrine and norepinephrine, which increases metabolic rate and temperature and fat utilization), and increase the expression of uncoupling protein in many tissues. Uncoupling protein is an enzyme that works to increase energy-wasting processes, creating more heat (calorie wasting or thermogenesis), rather than storing energy as fat.(34,23)
Ephedrine is another natural ingredient that, while effective at increasing weight loss (through decreased appetite and increased energy expenditure) and even maintaining muscle in the process, had a downside that would emerge if care was not taken in its use.(35,36) Many users have abused this supplement, using it for recreation or chronically using higher than recommended doses. In a highly politicized move, the FDA removed ephedrine from the market due to what it deemed excessive adverse events and undo risk to the public.(37,38,39)
Decreased Calorie Absorption
Lastly, we will look at supplements’ roles in reducing absorbed calories. Many dieters try to eat well, but the realities of eating out (someone else preparing food, social events and inaccurate portions or caloric information on food labels) can all lead to unexpected, unknown and unwanted energy intake. Supplements that inhibit absorption of a portion of ingested calories can give a "buffer zone" to one's daily food intake. Orlistat is a common prescription drug used to prevent the absorption of a portion of dietary fat.(40) However, gastrointestinal issues tend to make it unpopular for some and lead to a cessation of use.(41) The over-the-counter supplement Alli® is exactly the same as Orlistat, only at half the prescription dose per pill.
Phase 2® (a proprietary extract of the bean Phaseolus vulgaris) contains phaseolamin, which can block a portion of CHO absorption by blocking the action of alpha amylase, the enzyme that breaks down starch. Five hundred to 1000mgs of Phase 2 has been shown to dramatically reduce the absorption of starches thus calories, resulting in greater weight loss.(42,43) Subjects consuming a 2000-2200 calorie carbohydrate-rich diet and taking Phase 2 experienced ~700% greater weight loss than those using a placebo.
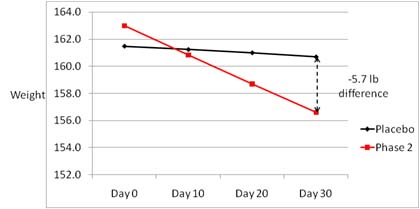
FIGURE 4: Subjects consumed a 2000-2200 calorie carbohydrate rich diet. The Phase 2 group experienced
~700% greater weight loss compared to the placebo.
The Role of Natural Substances in Weight Loss
As you can see, the mechanisms of appetite control can be rather complex. Most people attempting to lose weight realize that fewer calories need to be eaten, but maintaining the discipline necessary can be challenging. One's appetite is a big obstacle. Our desire to eat can be influenced by the many internal factors that regulate food intake and body weight as well as the overwhelming amount of external and environmental cues to eat. It does not help that food manufacturers and sellers are working diligently to ensure that you see and experience these cues to eat and buy their products at every turn. There is no way around the facts of weight loss: one must eat and absorb fewer calories than they burn on a regular basis. The good news is that there are safe, effective tools available to help you meet your goals and maintain your weight once you get there. They work by helping to increase the number of calories you burn, controlling the urge to eat, allowing you to feel full sooner and prohibiting a portion of consumed calories from being absorbed. If you‘ve got diet and exercise under control, these compounds make weight loss a little easier.
References
- Hunt SM, Groff JL. Advanced Nutrition and Human Metabolism. St. Paul, MN: West Publishing Company; 1990. 517pgs, pp411-414.
- Crowley VE. Overview of human obesity and central mechanisms regulating energy homeostasis. Ann Clin Biochem. 2008 May; 45(Pt3): 245-55.
- Small CJ, Bloom SR. Gut hormones and the control of appetite. Trends Endocrinol Metab. 2004 Aug; 15(6): 259-63.
- Hetherington MM. Cues to overeat: psychological factors influencing overconsumption. Proc Nutr Soc. 2007 Feb; 66(1): 113-23.
- Herman Cp, Polivy J. External Cues in the control of food intake in humans: the sensory-normative distinction. Physiol Behav. 2008 Aug ; 94(5): 722-8.
- Polivy J, Herman CP, Coelho JS. Caloric restriction in the presence of attractive food cues: external cues, eating and weight. Physiol Behav. 2008 Aug; 94(5): 729-33.
- Jansen A, Theunissen N, Slechten K, Nederkoorn C, Boon B, Mulken S, Roefs A. Overweight children overeat after exposure to food cues. Eat Behav. 2003 Aug. 4(2): 197-209.
- Jansen A, Vanreyten A, van Balveren T, Roefs A, Nederkoorn C, Havermans R. Negative affect and cue-induced overeating in non-eating disordered obesity. Appetite. 208 Nov; 51(3): 556-62.
- Halaas JL, Gajiwala KS, Maffei M, Cohen SL, Chait BT, Rabinowitz D, Lallone RL, Burley SK, Friedman JM Science. 1995 Jul 28;269(5223):543-6
- Ryan DH, Kaiser P, Bray GA. Sibutramine: a novel new agent for obesity treatment. Obes Res. 1995 Nov;3 Suppl 4:553S-559S.
- Inui A, Asakawa A, Bowers CY, et al (2004). "Ghrelin, appetite, and gastric motility: the emerging role of the stomach as an endocrine organ". FASEB J. 18 (3): 439–56.
- Gardiner JV, Jayasena CN, Bloom SR. Gut hormones: a weight off your mind. J Neuroendocrinol. 2008 Jun; 20(6): 834-41.
- Small CJ, Bloom SR. Gut hormones and the control of appetite. Trends Endocrinol Metab. 2004 Aug; 15(6): 259-53.
- Salas-Salvadó J, Farrés X, Luque X, Narejos S, Borrell M, Basora J, Anguera A, Torres F, Bulló M, Balanza R. Effect of two doses of a mixture of soluble fibres on body weight and metabolic variables in overweight patients: a randomized trial.
- Tiwary CM, Ward JA, Jackson BA. Effect of pectin on satiety in healthy US Army adults. J Am Coll Nutr. 1997 Oct;16(5):423-8.
- Vargo D, Doyle R, Floch MH.Colonic bacterial flora and serum cholesterol: alterations induced by dietary citrus pectin. Am J Gastroenterol. 1985 May;80(5):361-4.
- Astrup A, Breum L, Toubro S. Pharmacological and clinical studies of ephedrine and other thermogenic agonists. Obes Res. 1995 Nov;3 Suppl 4:537S-540S.
- Astrup A, Breum L, Toubro S, Hein P, Quaade F. The effect and safety of an ephedrine/caffeine compound compared to ephedrine, caffeine and placebo in obese subjects on an energy restricted diet. A double blind trial. Int J Obes Relat Metab Disord. 1992 Apr;16(4):269-77.
- Belza A, Toubro S, Astrup A. The effect of caffeine, green tea and tyrosine on thermogenesis and energy intake. Eur J Clin Nutr. 2007 Sep 19. [Epub ahead of print]
- Bérubé-Parent S, Pelletier C, Doré J, Tremblay A. Effects of encapsulated green tea and Guarana extracts containing a mixture of epigallocatechin-3-gallate and caffeine on 24 h energy expenditure and fat oxidation inmen. Br J Nutr. 2005 Sep;94(3):432-6.
- Westerterp-Plantenga MS, Smeets A, and Lejeune MP. Sensory and gastrointestinal satiety effects of capsaicin on food intake. Int J Obes 29:
- 682–688, 2005.
- Yoshioka M, Doucet E, Drapeau V, Dionne I, and Tremblay A.Combined effects of red pepper and caffeine consumption on 24 h energy balance in subjects given free access to foods. Br J Nutr 85: 203–211, 2001.
- Diepvens K, Westerterp KR, Westerterp-Plantenga MS. Obesity and thermogenesis related to the consumption of caffeine, ephedrine, capsaicin and green tea. Am J Physiol Regul Integr Comp Physiol. 2007 Jan;292(1):R77-85. Epub 2006 Jul 13
- Kuriyan R, Raj T, Srinivas SK, Vaz M, Rajendran R, Kurpad AV. Effect of Caralluma fimbriata extract on appetite, food intake and anthropometry in adult Indian men and women. Appetite. 2007 May;48(3):338-44. Epub 2006 Nov 13.
- Soni MG, Burdock GA, Preuss HG, Stohs SJ, Ohia SE, Bagchi D. Safety assessment of (-) –hydroxycitric acid and Super Citrimax ®, a novel
- calcium/potassium salt. Food and Chemical Toxicology (Accepted for publication)
- Jena BS, Jayaprakasha GK, Singh RP, Sakariah KK. Chemistry and biochemistry of (-)hydroxycitric acid from Garcinia. J Agric Food Chem 50:10-22, 2002.
- Astrup A, Toubro S, Cannon S, Hein P, Breum L, and Madsen J. Caffeine: a double-blind, placebo-controlled study of its thermogenic, metabolic, and cardiovascular effects in healthy volunteers. Am J Clin Nutr 51: 759–767, 1990
- Yoshida T, Sakane N, Umekawa T, and Kondo M. Relationship between basal metabolic rate, thermogenic response to caffeine, and body weight loss following combined low calorie and exercise treatment in obese women. Int J Obes 18: 345–350, 1994
- Bracco D, Ferrarra JM, Arnaud MJ, Jequier E, and Schutz Y. Effects of caffeine on energy metabolism, heart rate, and methylxanthines metabolism in lean and obese women. Am J Physiol Endocrinol Metab 269: E671–E678, 1995
- Dulloo AG, Duret C, Rohrer D, Girardier L, Mensi N, Fathi M, Chantre P, and Vandermander J. Efficacy of a green tea extract rich in catechin-polyphenols and caffeine in increasing 24-h energy expenditure and fat oxidation in humans. Am J Clin Nutr 70: 1040–1045, 1999
- Venables MC, Hulston CJ, Cox HR, Jeukendrup AE Green tea extract ingestion, fat oxidation and glucose tolerance in healthy humans.Am J Clin Nutr. 2008 Mar;87(3):778-84.
- Boschmann M, Thielecke F. The effects of epigallocatechin-3-gallate on thermogenesis and fat oxidation in obese men: a pilot study. J Am Coll Nutr. 2007 Aug;26(4):389S-395S.
- Brown AL, Lane J, Coverly J, Stocks J, Jackson S, Stephen A, Bluck L, Coward A, Hendrickx H. Effects of dietary supplementation with the green tea polyphenols epigallocatechin-3-gallate on insulin resistance and associated metabolic risk factors: randomized controlled trial.Br J Nutr. 2008 Aug 19:1-9. [Epub ahead of print]
- Yoshioka M, St-Pierre S, Drapeau V, Dionne I, Doucet E, Suzuki M, and Tremblay A. Effects of red pepper on appetite and energy intake. Br J Nutr 82: 115–123, 1999.
- Hallas J, Bjerrum L, Støvring H, Andersen M. Use of a prescribed ephedrine/caffeine combination and the risk of serious cardiovascular events: a registry-based case-crossover study. Am J Epidemiol. 2008 Oct 15;168(8):966-73. Epub 2008 Aug 27.
- Shekelle PG, Hardy ML, Morton SC, Maglione M, Mojica WA, Suttorp MJ, Rhodes SL, Jungvig L, Gagné J. JAMA. Efficacy and safety of ephedra and ephedrine for weight loss and athletic performance: a meta-analysis. 2003 Mar 26;289(12):1537-45. Epub 2003 Mar 10.
- Rados, Carol. "Ephedra Ban: No Shortage of Reasons." FDA U.S. Food and Drug Administration. 16 Oct 2008 http://www.fda.gov/FDAC/features/2004/204_ephedra.html.
- Thiessen, Mark. "Judge Rules Against FDA Ban on Ephedra". WashingtonPost.com. 15 Apr 2005. 16 Oct 2008. http://www.washingtonpost.com/wp-dyn/articles/A53586-2005Apr14.html.
- Duffy, Shannon P. "3rd Circuit Limits Appeal of FDA Ban of Ephedrine." LAW.COM. 9 Feb 2006. 16 Oct 2008. http://www.law.com/jsp/article.jsp?id=1139393111866.
- Sjöström L, Rissanen A, Andersen T, Boldrin M, Golay A, Koppeschaar HP, Krempf M. Lancet. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. European Multicentre Orlistat Study Group 1998 Jul 18;352(9123):167-72.
- Filippatos TD, Derdemezis CS, Gazi IF, Nakou ES, Mikhailidis DP, Elisaf MS. Orlistat-associated adverse effects and drug interactions: a critical review. Drug Saf. 2008;31(1):53-65.
- Celleno L, Tolaini MV, D'Amore A, Perricone NV, Preuss HG. A Dietary supplement containing standardized Phaseolus vulgaris extract influences body composition of overweight men and women. Int J Med Sci. 2007 Jan 24;4(1):45-52.
- Udani J, Singh BB. Blocking carbohydrate absorption and weight loss: a clinical trial using a proprietary fractionated white bean extract. Altern Ther Health Med. 2007 Jul-Aug;13(4):32-7.
- Abidov T, Grachev SV, Klimenov AL, Kalyuzhin OV. Effect of Rhododendron caucasicum extract on body weight and dietary lipids absorption in obese patients: a double-blind placebo controlled clinical study. Final report: Russian Ministry of Health; Grant: No 03-122-1997; Clinical Study; Project No: 0101-1997. 8 pp.
- Birari RB, Bhutani KK. Pancreatic lipase inhibitors from natural sources: unexplored potential. Drug Discov Today. 2007 Oct;12(19-20):879-89. Epub 2007 Sep 17.